
Videos
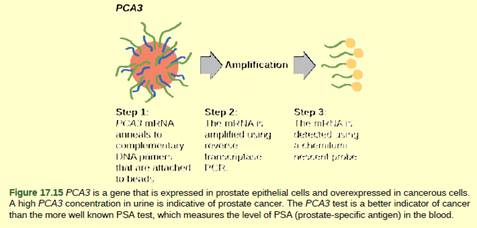
Figure 17.15 In 2011, the United States Preventative Services Task Force recommended against using the PSA test to screen healthy men for prostate cancer. Their recommendation is based on evidence that screening does not reduce the risk of death from prostate cancer. Prostate cancer often develops very slowly and does not cause problems, while the cancer treatment can have severe side effects. The PCA3 test is considered to be more accurate, but screening may still result in men who would not have been harmed by the cancer itself suffering side effects from treatment. What do you think? Should all healthy men be screened for prostate cancer using the PCA3 or PSA test? Should people in general be screened to find out if they have a genetic risk for cancer or other diseases?
Want to see the full answer?
Check out a sample textbook solution
Chapter 17 Solutions
Biology 2e
Additional Science Textbook Solutions
College Physics
Microbiology with Diseases by Body System (4th Edition)
Concepts of Genetics (12th Edition)
Microbiology: An Introduction (13th Edition)
Human Anatomy & Physiology (2nd Edition)
Genetic Analysis: An Integrated Approach (3rd Edition)


- Studies have shown that there are significant differences in cancer rates among different ethnic groups. For example, the Japanese have very high rates of colon cancer but very low rates of breast cancer. It has also been demonstrated that when members of low-risk ethnic groups move to high-risk areas, their cancer risks rise to those of the high-risk area. For example, Japanese who live in the United States, where the risk of breast cancer is high, have higher rates of breast cancer than do Japanese who live in Japan. What are some of the possible explanations for this phenomenon? What factors may explain why the Japanese have higher rates of colon cancer than do other ethnic groups?arrow_forwardIn a Cervical Cancer screening program, 500 asymptomatic women were examined using the Pap smear test. 200 of the women who truly had lesions were correctly classified; 14 with lesions were wrongly classified as negative. 253 women who had no lesions were correctly classified; 33 women with no lesions were wrongly reported as positive. (A) Summarise the information provided in an appropirate table. (B) Based on the information above, calculate the Sensitivity, Specificity, Positive and Negative Predictive Values of the Pap smear test.arrow_forwardthe task is to use this image to write a results section of a report about: Identification of Differentially Expressed Genes in Breast Cancer Using RNA-Seq. 1000 words would be bestarrow_forward
- How can genetic testing help in cancer diagnosis? Answer specificallyarrow_forwardIf improved diagnostic tests are developed from this project, is the effort worth it if the cancers diagnosed have no treatment available?arrow_forwardYou are in charge of a new gene therapy clinic. Two cases have been referred to you for review and possible therapy. Case 1. A mutation in the promoter of a proto-oncogene causes the gene to make too much of its normal product, a receptor protein that promotes cell division. The uncontrolled cell division has caused cancer. Case 2. A mutation in an exon of a tumor-suppressor gene makes this gene nonfunctional. The product of this gene normally suppresses cell division. The mutant gene cannot suppress cell division, and this has led to cancer. What treatment options can you suggest for each case?arrow_forward
- Benign tumors: a. are noncancerous growths that do not spread to other tissues b. do not contain mutations c. are malignant and clonal in origin d. metastasize to other tissues e. none of thesearrow_forwardThe most common therapeutic approaches to treating cancer include all of the following except ________. a. chemotherapy b. irradiation of tumors c. surgery to remove cancerous tissue d. administering doses of vitaminsarrow_forwardSurgery remains a mainstay in the treatment of many forms of cancer, but it is no longer used in diagnosis due to the risks associated with surgery and improved nonsurgical diagnostic methods. True Falsearrow_forward
- In 2019, a study of the adverse effects of x-rays on subsequent cancer among children was done using records from several large children’s hospitals from 1990 to 1995. 10,000 children were selected as a representative population of ill children seen at the hospitals during that time. Subjects were classified according to whether or not they received an x-ray during their stay in the hospital and were followed from their hospital stay through 2019 for cancer development. During the follow-up period, 49 incident cancers occurred in 3,263 children who had received an x-ray, and 47 incident cancers occurred in the 6,737 children who had not received an x-ray during their hospitalization. What is the risk difference of developing cancer comparing children who had an x-ray to those who did not? a) 6 excess cases per 1000 b) 2 excess cases per 1000 c) 8 excess cases per 1000arrow_forwardWhat are tumor markers? Describe major types of tumor markers used in breast cancer care. Can tumor markers be used in breast cancer screening?use your own wordsarrow_forwardDescribe one chemotherapeutic approach that can be used to treat prostate cancer? Your answer should include information about the molecular processes and interactions which are at the core of the treatment strategyarrow_forward
- Biology 2eBiologyISBN:9781947172517Author:Matthew Douglas, Jung Choi, Mary Ann ClarkPublisher:OpenStax
 Human Heredity: Principles and Issues (MindTap Co...BiologyISBN:9781305251052Author:Michael CummingsPublisher:Cengage Learning
Human Heredity: Principles and Issues (MindTap Co...BiologyISBN:9781305251052Author:Michael CummingsPublisher:Cengage Learning
 Human Biology (MindTap Course List)BiologyISBN:9781305112100Author:Cecie Starr, Beverly McMillanPublisher:Cengage Learning
Human Biology (MindTap Course List)BiologyISBN:9781305112100Author:Cecie Starr, Beverly McMillanPublisher:Cengage Learning